Pharmacotherapeutic group: Therapeutic radiopharmaceuticals, Other therapeutic radiopharmaceuticals.
ATC code: V10XX05.
Pharmacology: Pharmacodynamics: Mechanism of action: The active moiety of Pluvicto is the radionuclide lutetium-177 which is linked to a small-molecule ligand that targets and binds with high affinity to PSMA, a transmembrane protein that is highly expressed in prostate cancer, including mCRPC. Upon the binding of Pluvicto to PSMA-expressing cancer cells, the beta-minus emission from lutetium-177 delivers therapeutic radiation to the targeted cell, as well as to surrounding cells, and induces DNA damage which can lead to cell death.
Pharmacodynamic effects: Unlabelled vipivotide tetraxetan does not have any pharmacodynamic activity.
Clinical efficacy and safety: VISION: The efficacy of Pluvicto in patients with progressive, PSMA-positive mCRPC was evaluated in VISION, a randomised, multicentre, open-label phase III study. Eight hundred and thirty-one (N=831) adult patients were randomised (2:1) to receive either Pluvicto 7400 MBq every 6 weeks for up to a total of 6 doses plus best standard of care (BSoC) (N=551) or BSoC alone (N=280). Patients who received 4 doses of Pluvicto were reassessed for evidence of response, signs of residual disease, and tolerability and could receive up to 2 additional doses per physician's discretion.
To maintain castration status, all patients continued to receive a GnRH analogue or had prior bilateral orchiectomy. Eligible patients were required to have progressive, PSMA-positive mCRPC, Eastern Cooperative Oncology Group (ECOG) performance status (PS) of 0 to 2, at least one metastatic lesion present on computed tomography (CT), magnetic resonance imaging (MRI) or bone scan imaging, and adequate renal, hepatic and haematological function.
Eligible patients were also required to have received at least one AR pathway inhibitor, such as abiraterone acetate or enzalutamide, and 1 or 2 prior taxane-based chemotherapy regimens (with a regimen defined as a minimum exposure of 2 cycles of a taxane). Patients treated with only 1 prior taxane-based chemotherapy regimen were eligible if the patient was unwilling or the physician deemed the patient unsuitable to receive a second regimen. Patients with unstable symptomatic central nervous system metastases or symptomatic or clinically/radiologically impending spinal cord compression were not eligible for the study. Patients underwent a gallium (
68Ga) gozetotide positron emission tomography (PET) scan to evaluate PSMA expression in lesions defined by central read criteria. Eligible patients were required to have PSMA-positive mCRPC defined as having at least one tumour lesion with gallium (
68Ga) gozetotide uptake greater than in normal liver. Patients were excluded if any lesions exceeding size criteria in short axis (organs ≥1 cm, lymph nodes ≥2.5 cm, bones [soft-tissue component] ≥1 cm) had uptake less than or equal to uptake in normal liver.
BSoC administered at the physician's discretion included: supportive measures including pain management, hydration, blood transfusions, etc.; ketoconazole; radiation therapy (including seeded form or any external beam radiotherapy [including stereotactic body radiotherapy and palliative external beam]) to localised prostate cancer targets; bone-targeted agents including zoledronic acid, denosumab and any bisphosphonates; androgen-reducing agents including GnRH analogues, any corticosteroid, and 5-alpha reductases; AR pathway inhibitors. BSoC excluded investigational agents, cytotoxic chemotherapy, immunotherapy, other systemic radioisotopes and hemi-body radiotherapy treatment.
Patients continued randomised treatment until evidence of tumour progression (based on investigator assessment per Prostate Cancer Working Group 3 [PCWG3] criteria), unacceptable toxicity, use of prohibited treatment, non-compliance or withdrawal, or lack of clinical benefit.
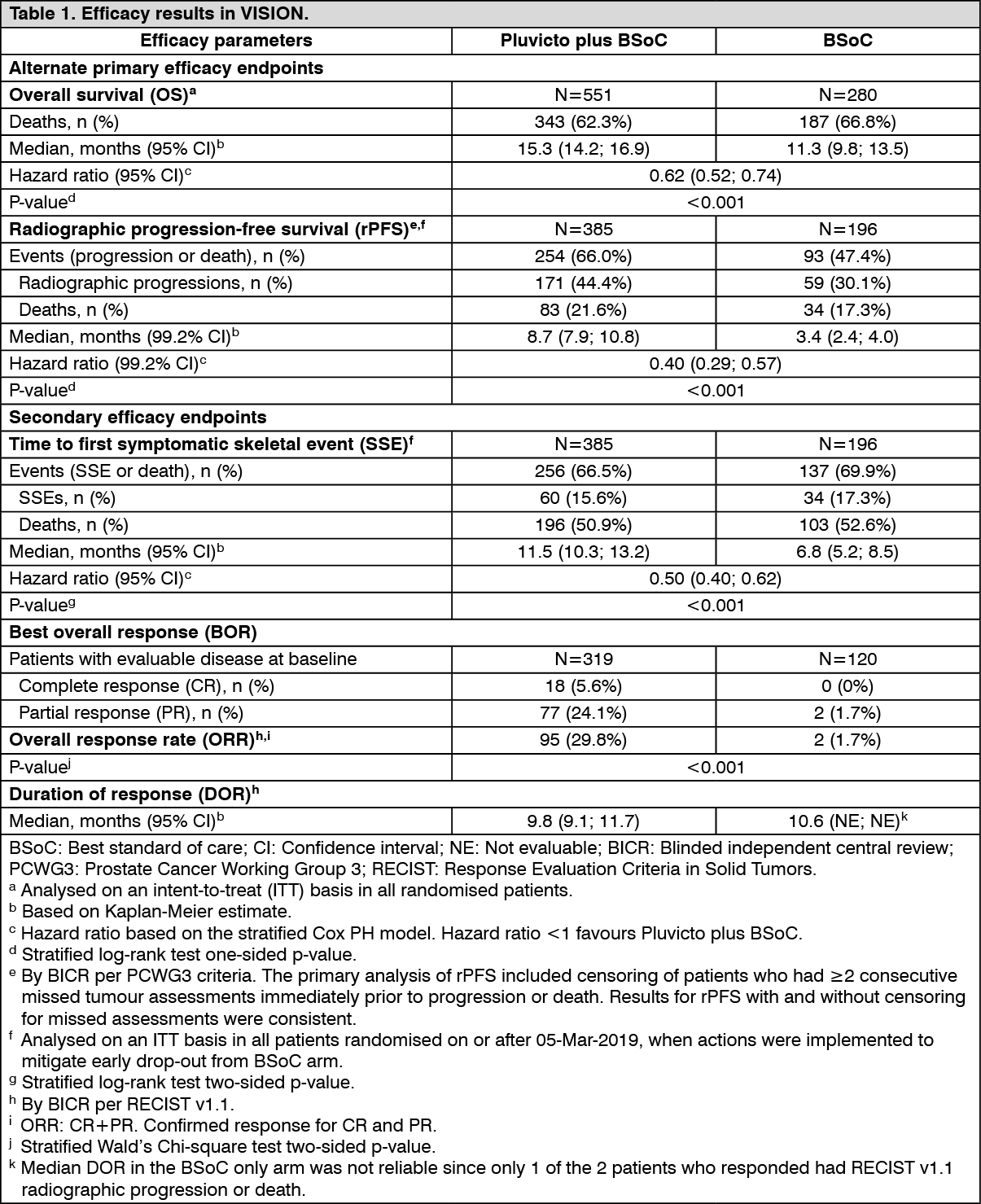
The primary efficacy endpoints were overall survival (OS) and radiographic progression-free survival (rPFS) as determined by blinded independent central review (BICR) per PCWG3 criteria. Among the secondary efficacy endpoints were overall response rate (ORR) as determined by BICR per Response Evaluation Criteria in Solid Tumors (RECIST) v1.1 and time to first symptomatic skeletal event (SSE) defined as first new symptomatic pathological bone fracture, spinal cord compression, tumour-related orthopaedic surgical intervention, requirement for radiation therapy to relieve bone pain, or death from any cause, whichever occurred first. Radiographic imaging for tumour assessment (CT with contrast/MRI imaging and bone scan) was done every 8 weeks (±4 days) after the first dose for the first 24 weeks (independent of dose delays), then every 12 weeks (±4 days).
Demographic and baseline disease characteristics were balanced between the treatment arms. The median age was 71 years (range: 40 to 94 years); 86.8% White; 6.6% Black or African American; 2.4% Asian; 92.4% had ECOG PS0-1; 7.6% had ECOG PS2. Randomisation was stratified by baseline lactate dehydrogenase (LDH ≤260 IU/L vs. >260 IU/L), presence of liver metastases (yes vs. no), ECOG PS score (0 or 1 vs. 2), and inclusion of an AR pathway inhibitor as part of BSoC at the time of randomisation (yes vs. no). At randomisation, all patients (100.0%) had received at least one prior taxane-based chemotherapy regimen and 41.2% of patients had received two; 97.1% of patients had received docetaxel and 38.0% of patients had received cabazitaxel. At randomisation, 51.3% of patients had received one prior AR pathway inhibitor, 41.0% of patients had received 2, and 7.7% of patients had received 3 or more. During the randomised treatment period, 52.6% of patients in the Pluvicto plus BSoC arm and 67.8% of patients in the BSoC alone arm received at least one AR pathway inhibitor.
Efficacy results for VISION are presented in Table 1 and Figures 1 and 2. The final analyses of OS and rPFS were event-driven and conducted after the occurrence of 530 deaths and 347 events, respectively. (See Table 1 and Figures 1 and 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Paediatric population:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Paediatric population: The European Medicines Agency has waived the obligation to submit the results of studies with Pluvicto in all subsets of the paediatric population in the treatment of PSMA-expressing prostate cancer (see Dosage & Administration for information on paediatric use).
Pharmacokinetics: The pharmacokinetics of lutetium (
177Lu) vipivotide tetraxetan have been characterised in 30 patients in the phase III VISION sub-study.
Absorption: Pluvicto is administered intravenously and is immediately and completely bioavailable.
The geometric mean blood exposure (area under the curve [AUC
inf]) for lutetium (
177Lu) vipivotide tetraxetan at the recommended dose is 52.3 ng·h/mL (geometric mean coefficient of variation [CV] 31.4%). The geometric mean maximum blood concentration (C
max) for lutetium (
177Lu) vipivotide tetraxetan is 6.58 ng/mL (CV 43.5%).
Distribution: The geometric mean volume of distribution (V
z) for lutetium
(177Lu) vipivotide tetraxetan is 123 L (CV 78.1%).
Unlabelled vipivotide tetraxetan and non-radioactive lutetium (
175Lu) vipivotide tetraxetan are each 60% to 70% bound to human plasma proteins.
Organ uptake: The biodistribution of lutetium (
177Lu) vipivotide tetraxetan shows primary uptake in lacrimal glands, salivary glands, kidneys, urinary bladder wall, liver, small intestine and large intestine (left and right colon).
Elimination: The geometric mean clearance (CL) for lutetium (
177Lu) vipivotide tetraxetan is 2.04 L/h (CV 31.5%).
Lutetium (
177Lu) vipivotide tetraxetan is primarily eliminated renally.
Half-life: Pluvicto shows a bi-exponential elimination with a geometric mean terminal elimination half-life (t
½) of 41.6 hours (CV 68.8%).
Biotransformation: Lutetium (
177Lu) vipivotide tetraxetan does not undergo hepatic or renal metabolism.
In vitro evaluation of drug interaction potential: CYP450 enzymes: Vipivotide tetraxetan is not a substrate of cytochrome P450 (CYP450) enzymes. It does not induce cytochrome P450 (CYP) 1A2, 2B6 or 3A4, and it does not inhibit cytochrome P450 (CYP) 1A2, 2B6, 2C8, 2C9, 2C19, 2D6 or 3A4/5
in vitro.
Transporters: Vipivotide tetraxetan is not a substrate of BCRP, P-gp, MATE1, MATE2-K, OAT1, OAT3 or OCT2, and it is not an inhibitor of BCRP, P-gp, BSEP, MATE1, MATE2-K, OAT1, OAT3, OATP1B1, OATP1B3, OCT1 or OCT2
in vitro.
Special populations: Effects of age and body weight: No clinically significant effects on the pharmacokinetic parameters of lutetium (
177Lu) vipivotide tetraxetan were identified for the following covariates assessed in 30 patients in the phase III VISION sub-study: age (median: 67 years; range: 52 to 80 years) and body weight (median: 88.8 kg; range: 63.8 to 143.0 kg).
Renal impairment: Exposure (AUC) of lutetium (
177Lu) vipivotide tetraxetan increased by 20% in patients with mild renal impairment compared to normal renal function. Kidney dosimetry half-life also increased in patients with mild renal impairment compared to normal renal function, 51 hours vs. 37 hours, respectively. Patients with mild or moderate renal impairment may be at greater risk of toxicity (see Precautions). No pharmacokinetic data are available for patients with moderate to severe renal impairment with baseline CLcr <50 mL/min or end-stage renal disease.
Toxicology: Preclinical safety data: No toxicological effects were observed in safety pharmacology or single-dose toxicity studies in rats and minipigs administered a non-radioactive formulation containing unlabelled vipivotide tetraxetan and lutetium (
175Lu) vipivotide tetraxetan, or in repeat-dose toxicity studies in rats administered unlabelled vipivotide tetraxetan.
Carcinogenicity and mutagenicity: Mutagenicity and long-term carcinogenicity studies have not been carried out with lutetium (
177Lu) vipivotide tetraxetan; however, radiation is a carcinogen and mutagen.
Dosimetry: Radiation dose to specific organs, which may not be the target organ of therapy, can be influenced significantly by pathophysiological changes induced by the disease process. This should be taken into consideration when using the following information.
Dosimetry of lutetium (
177Lu) vipivotide tetraxetan was collected in 29 patients in the phase III VISION sub-study, in order to calculate whole body and organ radiation dosimetry. The mean and standard deviation (SD) of the estimated absorbed doses to different organs for adult patients receiving Pluvicto are shown in Table 2. The organs with the highest absorbed doses are lacrimal glands and salivary glands. (See Table 2.)
The maximum penetration of lutetium-177 in tissue is approximately 2 mm and the mean penetration is 0.67 mm.
Click on icon to see table/diagram/image





 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image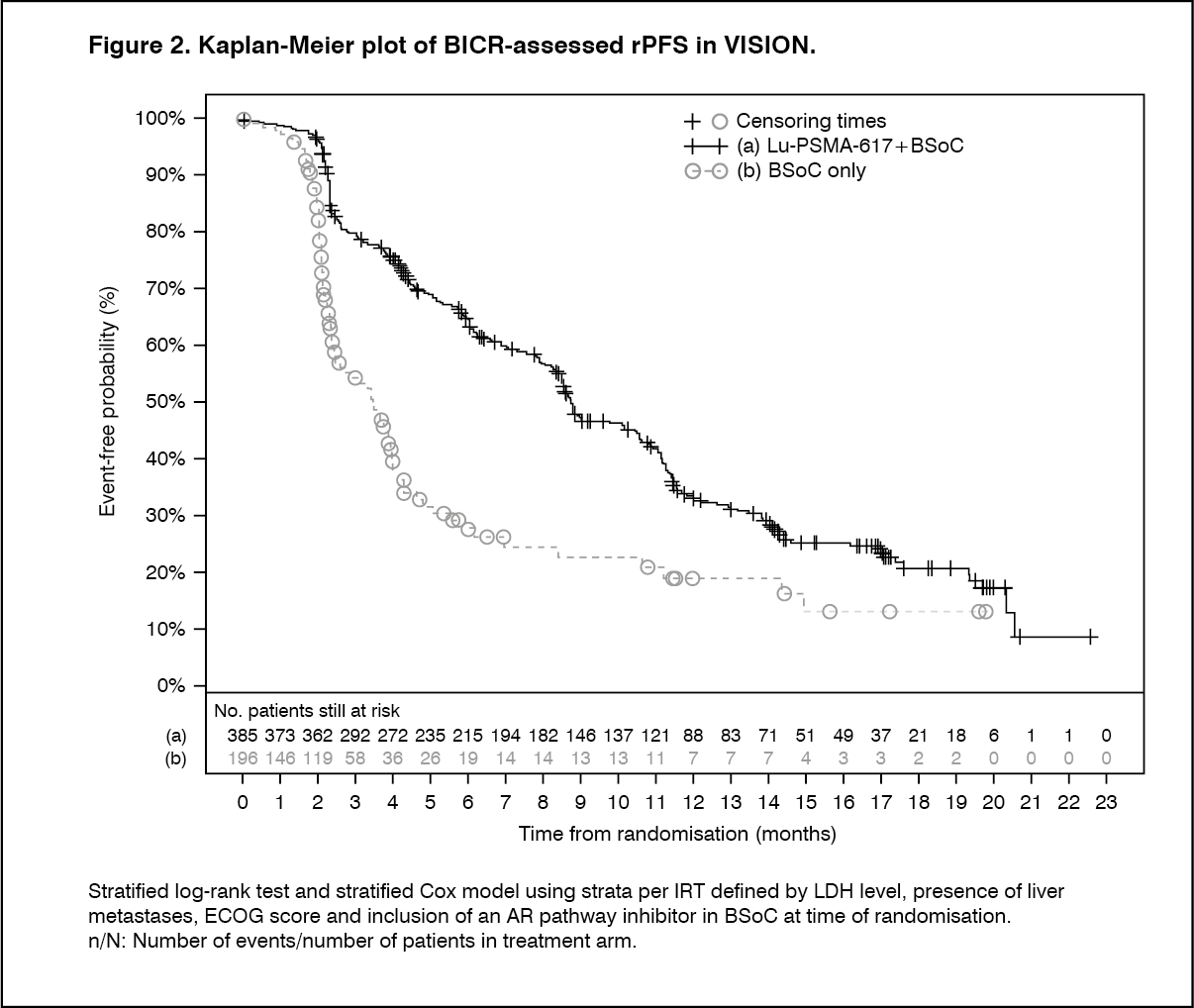 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image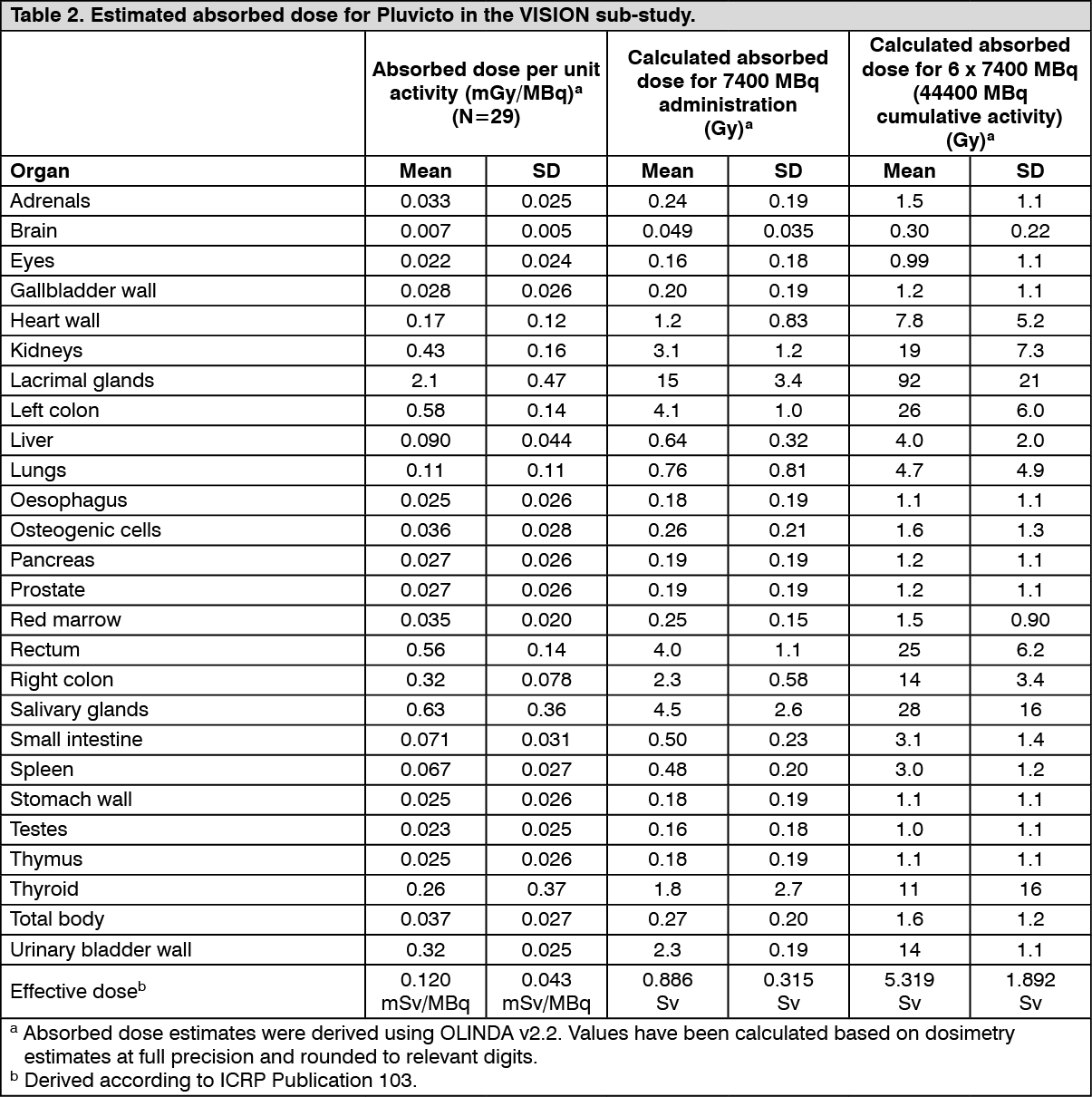 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image

 Sign Out
Sign Out
