


 Sign Out
Sign Out




Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
The data described as follows reflect exposure to Nilemdo in two placebo-controlled trials that included 2009 patients treated with Nilemdo for 52 weeks (median treatment duration of 52 weeks) [see Pharmacology: Pharmacodynamics: Clinical Studies under Actions]. The mean age for Nilemdo-treated patients was 65.4 years, 29% were women, 3% were Hispanic, 95% White, 3% Black, 1% Asian, and 1% other races. All patients received Nilemdo 180 mg orally once daily plus maximally tolerated statin therapy alone or in combination with other lipid-lowering therapies. At baseline, 97% of patients had clinical atherosclerotic cardiovascular disease (ASCVD) and about 4% had a diagnosis of heterozygous familial hypercholesterolemia (HeFH). Patients on simvastatin 40 mg/day or higher were excluded from the trials.
Adverse reactions led to discontinuation of treatment in 11% of Nilemdo-treated patients and 8% of placebo-treated patients. The most common reasons for Nilemdo treatment discontinuation were muscle spasms (0.5% versus 0.3% placebo), diarrhea (0.4% versus 0.1% placebo), and pain in extremity (0.3% versus 0.0% placebo). Adverse reactions reported in at least 2% of Nilemdo-treated patients and more frequently than in placebo-treated patients are shown in Table 3. (See Table 3.)
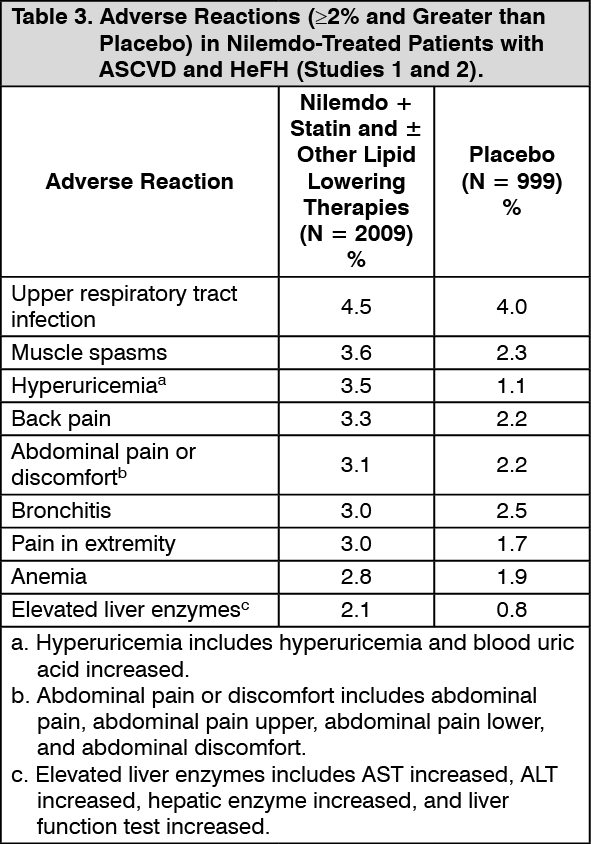 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTendon Rupture: Nilemdo was associated with an increased risk of tendon rupture, occurring in 0.5% of Nilemdo-treated patients versus 0% of placebo-treated patients.
Gout: Nilemdo was associated with an increased risk of gout, occurring in 1.5% of Nilemdo-treated patients versus 0.4% of placebo-treated patients.
Benign Prostatic Hyperplasia: Nilemdo was associated with an increased risk of benign prostatic hyperplasia (BPH) or prostatomegaly in men with no reported history of BPH, occurring in 1.3% of Nilemdo-treated patients versus 0.1% of placebo-treated patients. The clinical significance is unknown.
Atrial Fibrillation: Nilemdo was associated with an imbalance in atrial fibrillation, occurring in 1.7% of Nilemdo-treated patients versus 1.1% of placebo-treated patients.
Laboratory Tests: Nilemdo was associated with persistent changes in multiple laboratory tests within the first 4 weeks of treatment. Laboratory test values returned to baseline following discontinuation of treatment.
Increase in Creatinine and Blood Urea Nitrogen: Overall, there was a mean increase in serum creatinine of 0.05 mg/dL compared to baseline with Nilemdo at Week 12. Approximately 3.8% of patients treated with Nilemdo had blood urea nitrogen values that doubled (versus 1.5% placebo), and about 2.2% of patients had creatinine values that increased by 0.5 mg/dL (versus 1.1% placebo).
Decrease in Hemoglobin and Leukocytes: Approximately 5.1% of patients (versus 2.3% placebo) had decreases in hemoglobin levels of 2 or more g/dL and below the lower limit of normal on one or more occasion. Anemia was reported in 2.8% of patients treated with Nilemdo and 1.9% of patients treated with placebo. Hemoglobin decrease was generally asymptomatic and did not require medical intervention. Decreased leukocyte count was also observed. Approximately 9.0% of Nilemdo-treated patients with normal baseline leukocyte count had a decrease to less than the lower limit of normal on one or more occasion (versus 6.7% placebo). Leukocyte decrease was generally asymptomatic and did not require medical intervention. In clinical trials, there was a small imbalance in skin or soft tissue infections, including cellulitis (0.8% versus 0.4%), but there was no imbalance in other infections.
Increase in Platelet Count: Approximately 10.1% of patients (versus 4.7% placebo) had increases in platelet counts of 100 × 109/L or more on one or more occasion. Platelet count increase was asymptomatic, did not result in increased risk for thromboembolic events, and did not require medical intervention.
Increase in Liver Enzymes: Increases in hepatic transaminases (AST and/or ALT) were observed with Nilemdo. In most cases, the elevations were transient and resolved or improved with continued therapy or after discontinuation of therapy. Increases to more than 3× the upper limit of normal (ULN) in AST occurred in 1.4% of patients treated with Nilemdo versus 0.4% of placebo patients, and increases to more than 5× ULN occurred in 0.4% of Nilemdo-treated versus 0.2% of placebo-treated patients. Increases in ALT occurred with similar incidence between Nilemdo- and placebo-treated patients. Elevations in transaminases were generally asymptomatic and not associated with elevations ≥2× ULN in bilirubin or with cholestasis.
Increase in Creatine Kinase: Approximately 1.0% of patients (versus 0.6% placebo) had elevations of CK levels of 5 or more times the normal value on one or more occasions, and 0.4% of patients (versus 0.2% placebo) had elevations of CK levels of 10 or more times.
View ADR Monitoring Form