


 Sign Out
Sign Out




Clinical Trials Experience: Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice.
Bempedoic acid: The data described as follows reflect exposure to bempedoic acid in two placebo-controlled trials that included 2009 patients treated with bempedoic acid for 52 weeks (median treatment duration of 52 weeks) [see Pharmacology: Pharmacodynamics: Clinical Studies under Actions]. The mean age for bempedoic acid-treated patients was 65.4 years, 29% were women, 3% were Hispanic, 95% White, 3% Black, 1% Asian, and 1% other races. All patients received bempedoic acid 180 mg orally once daily plus maximally tolerated statin therapy alone or in combination with other lipid-lowering therapies. At baseline, 97% of patients had clinical atherosclerotic cardiovascular disease (ASCVD) and about 4% had a diagnosis of heterozygous familial hypercholesterolemia (HeFH). Patients on simvastatin 40 mg/day or higher were excluded from the trials.
Adverse reactions led to discontinuation of treatment in 11% of bempedoic acid-treated patients and 8% of placebo-treated patients. The most common reasons for bempedoic acid treatment discontinuation were muscle spasms (0.5% versus 0.3% placebo), diarrhea (0.4% versus 0.1% placebo), and pain in extremity (0.3% versus 0.0% placebo). Adverse reactions reported in at least 2% of bempedoic acid-treated patients and more frequently than in placebo-treated patients are shown in Table 2. (See Table 2.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageTendon Rupture: Bempedoic acid was associated with an increased risk of tendon rupture, occurring in 0.5% of bempedoic acid-treated patients versus 0% of placebo-treated patients.
Gout: Bempedoic acid was associated with an increased risk of gout, occurring in 1.5% of bempedoic acid-treated patients versus 0.4% of placebo-treated patients.
Benign Prostatic Hyperplasia: Bempedoic acid was associated with an increased risk of benign prostatic hyperplasia (BPH) or prostatomegaly in men with no reported history of BPH, occurring in 1.3% of bempedoic acid-treated patients versus 0.1% of placebo-treated patients. The clinical significance is unknown.
Atrial Fibrillation: Bempedoic acid was associated with an imbalance in atrial fibrillation, occurring in 1.7% of bempedoic acid-treated patients versus 1.1% of placebo-treated patients.
Laboratory Tests: Bempedoic acid was associated with persistent changes in multiple laboratory tests within the first 4 weeks of treatment. Laboratory test values returned to baseline following discontinuation of treatment.
Increase in Creatinine and Blood Urea Nitrogen: Overall, there was a mean increase in serum creatinine of 0.05 mg/dL compared to baseline with bempedoic acid at Week 12. Approximately 3.8% of patients treated with bempedoic acid had blood urea nitrogen values that doubled (versus 1.5% placebo), and about 2.2% of patients had creatinine values that increased by 0.5 mg/dL (versus 1.1% placebo).
Decreased Hemoglobin and Leukocytes: Approximately 5.1% of patients treated with bempedoic acid (versus 2.3% placebo) had decreases in hemoglobin levels of 2 or more g/dL and below the lower limit of normal on one or more occasion. Anemia was reported in 2.8% of patients treated with bempedoic acid and 1.9% of patients treated with placebo. Hemoglobin decrease was generally asymptomatic and did not require medical intervention. Decreased leukocyte count was also observed. Approximately 9.0% of bempedoic acid-treated patients with normal baseline leukocyte count had a decrease to less than the lower limit of normal on one or more occasion (versus 6.7% placebo). Leukocyte decrease was generally asymptomatic and did not require medical intervention. In clinical trials, there was a small imbalance in skin or soft tissue infections, including cellulitis (0.8% versus 0.4%), but there was no imbalance in other infections.
Increase in Platelet Count: Approximately 10.1% of bempedoic acid-treated patients (versus 4.7% placebo) had increases in platelet counts of 100 × 109/L or more on one or more occasion. Platelet count increase was asymptomatic, did not result in increased risk for thromboembolic events, and did not require medical intervention.
Increase in Liver Enzymes: Increases in hepatic transaminases (AST and/or ALT) were observed with bempedoic acid. In most cases, the elevations were transient and resolved or improved with continued therapy or after discontinuation of therapy. Increases to more than 3× the upper limit of normal (ULN) in AST occurred in 1.4% of patients treated with bempedoic acid versus 0.4% of placebo patients, and increases to more than 5× ULN occurred in 0.4% of bempedoic acid-treated versus 0.2% of placebo-treated patients. Increases in ALT occurred with similar incidence between bempedoic acid- and placebo-treated patients. Elevations in transaminases were generally asymptomatic and not associated with elevations ≥2× ULN in bilirubin or with cholestasis.
Increase in Creatine Kinase: Approximately 1.0% of patients (versus 0.6% placebo) had elevations of CK levels of 5 or more times the normal value on one or more occasions, and 0.4% of patients (versus 0.2% placebo) had elevations of CK levels of 10 or more times.
Ezetimibe: In 10 double-blind, placebo-controlled clinical trials, 2396 patients with primary hyperlipidemia (age range 9-86 years, 50% women, 90% Caucasians, 5% Blacks, 3% Hispanics, 2% Asians) and elevated LDL-C were treated with ezetimibe 10 mg/day for a median treatment duration of 12 weeks (range 0 to 39 weeks).
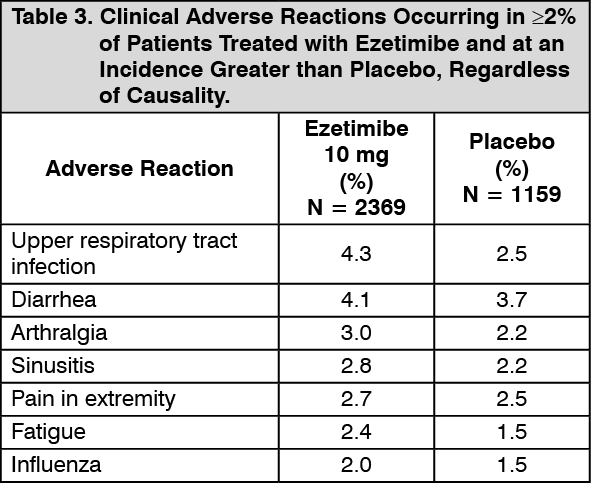
Adverse reactions led to discontinuation of treatment in 3.3% of ezetimibe-treated patients and 2.9% of placebo-treated patients. The most common reasons for ezetimibe treatment discontinuation were arthralgia (0.3%), dizziness (0.2%), and gamma-glutamyltransferase increased (0.2%). Adverse reactions reported in ≥2% of patients treated with ezetimibe and at an incidence greater than placebo in placebo-controlled studies of ezetimibe, regardless of causality assessment, are shown in Table 3. (See Table 3.)
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/imageThe frequency of less common adverse reactions was comparable between ezetimibe and placebo.
Nustendi: In a 4-arm, 12-week, randomized, double-blind, placebo-controlled, parallel group, factorial trial, 85 patients received Nustendi (180 mg of bempedoic acid and 10 mg of ezetimibe) once daily [see Pharmacology: Pharmacodynamics: Clinical Studies under Actions]. The mean age for Nustendi-treated patients was 62 years, 51% were women, 12% Hispanic, 78% White, 19% Black, and 2% Asian. At baseline, 61% of patients had clinical atherosclerotic cardiovascular disease (ASCVD) and/or a diagnosis of heterozygous familial hypercholesterolemia. All patients received Nustendi plus maximally tolerated statin therapy. Patients taking simvastatin 40 mg/day or higher and patients taking non-statin lipid-lowering therapy (including fibrates, niacin, bile acid sequestrants, ezetimibe, and PCSK9 inhibitors) were excluded from the trial.
Adverse reactions led to discontinuation of treatment in 8% of patients on Nustendi, 5% of patients on placebo, 10% of patients on bempedoic acid, and 12% of patients on ezetimibe. The most common reason for Nustendi treatment discontinuation was oral discomfort (2% Nustendi versus 0% placebo). The most commonly reported adverse reactions (incidence ≥3% and greater than placebo) observed with Nustendi, but not observed in clinical trials of bempedoic acid or ezetimibe, were urinary tract infection (5.9% Nustendi versus 2.4% placebo), nasopharyngitis (4.7% Nustendi versus 0% placebo), and constipation (4.7% Nustendi versus 0% placebo).
Post-marketing Experience: Because these reactions are reported voluntarily from a population of uncertain size, it is generally not possible to reliably estimate their frequency or establish a causal relationship to drug exposure.
The following additional adverse reactions have been reported in post-marketing experience for ezetimibe: Hypersensitivity reactions, including anaphylaxis, angioedema, rash, and urticaria; erythema multiforme; myalgia; elevated creatine phosphokinase; myopathy/rhabdomyolysis; elevations in liver transaminases; hepatitis; abdominal pain; thrombocytopenia; pancreatitis; nausea; dizziness; paresthesia; depression; headache; cholelithiasis; cholecystitis.
View ADR Monitoring Form